Coronavirus
Technology Solutions
December 29, 2020
Vaccine for Poor
Countries will
Save $466
billion in Ten
Wealthy
Countries
Vaccine Efficacy
May Be Short
Term
New Virus
Variants in Many
Countries
Holistic Plan
to Battle COVID
for 1.7 Billion
Students
____________________________________________________________________________
Vaccine for Poor
Countries will
Save $466
billion in Ten
Wealthy
Countries
There are major
negative
economic
consequences for
wealthy
countries if
poorer ones do
not get the
vaccines they
need. Global
equitable access
to COVID-19
vaccines is
estimated to
generate
economic
benefits of at
least $153
billion in
2020–21, and
$466 billion by
2025, in 10
major economies.
This is the
conclusion
according to new
report by the
Eurasia Group
It finds that
leaving low-and
lower-middle-income
countries
(LLMICs) without
access to
vaccines amid
the COVID-19
pandemic will
cause
significant
economic damage
that puts
decades of
economic
progress at risk
– for both
LLMICs and
advanced
economies
alike.
The report by
the Eurasia
Group analyses
ten major
economies –
Canada, France,
Germany, Japan,
Qatar, South
Korea, Sweden,
United Arab
Emirates, United
Kingdom and the
United States –
to assess the
economic
benefits to
advanced
economies of
contributing to
the work of
the Access to
COVID-19 Tools
(ACT)
Accelerator.
The ACT
Accelerator, led
by WHO and
partnering with
the world’s
leading
international
health
organizations,
is a unique
global
collaboration
which supports
the development
and equitable
distribution of
the tests,
treatments, and
vaccines the
world needs to
fight COVID-19.
However, the
programme still
has a
significant
funding gap of
$28.2 billion –
with $4.3
billion needed
urgently to
fast-track
critical areas
of work. If that
shortfall isn’t
met, low- and
low-middle
income countries
will have
delayed access
to these vital
tools in 2021,
which will
result in a
protracted
pandemic, with
severe economic
consequences,
not just for
these countries
by also for the
wider global
economy.
The report,
which was
commissioned by
the Bill &
Melinda Gates
Foundation,
finds that the
economic
benefits of a
global equitable
vaccine solution
alone for the 10
countries
included in the
analysis would
be at least $153
billion in
2020-21, rising
to $466 billion
by 2025. This is
more than 12
times the $38
billion
estimated total
cost of the ACT
Accelerator.
This figure was
compiled using
the expected
negative effects
of sustained
coronavirus
outbreaks in
LLMICs, based on
the downside and
baseline
scenarios of
the IMF’s
October 2020
World Economic
Outlook forecasts.
So far, the 10
countries
featured in the
report have
contributed $2.4
billion to the
work of the ACT
Accelerator,
with the United
Kingdom
committing just
over $1 billion,
and Germany,
Canada, Japan
and France
committing $618
million, $290
million, $229
million and $147
million
respectively.
In just seven
months, the ACT
Accelerator’s
progress has
been
significant:
over 50
diagnostic tests
have been
evaluated and
new rapid
antigen
diagnostics have
been developed
and being made
available for
LMICs;
life-saving
Dexamethasone
treatments are
being rolled
out, research
into monoclonal
antibody
treatments is
advancing; and
through the
Health Systems
Connector, the
health system
requirements for
delivery of
COVID-19 tools
have been mapped
in 4 out of 6
world regions.
COVAX, the
Vaccines Pillar
of the ACT
Accelerator, has
the world’s
largest and most
diverse
portfolio of
vaccines. It
aims to
accelerate the
development and
manufacture of
COVID-19
vaccines, and to
guarantee fair
and equitable
access for every
participating
country. Working
with 189
countries, COVAX
is supporting
the development
of nine vaccine
candidates
through CEPI, 8
of which are in
clinical trials.
COVAX has
secured hundreds
of millions of
doses of three
promising
candidates,
including at
least 200
million doses
for LICs, with
the support of
the Bill &
Melinda Gates
Foundation.
This new report
emphasizes the
funding urgency
and the return
on investment
for donor
countries of the
work of the ACT
Accelerator,
which published
its Urgent
Priorities and
Financing
Requirements on
10 November.
Dr Tedros
Adhanom
Ghebreyesus, WHO
Director-General,
called on
countries to
commit to the
work of the ACT
Accelerator,
stating that,
“The ACT
Accelerator is
the global
solution to
ending the acute
phase of the
pandemic as
quickly as
possible by
ensuring
equitable access
to COVID-19
tools.
Contributing to
the ACT
Accelerator it
is not just the
right thing to
do – it’s the
smart thing for
all countries –
socially,
economically and
politically.”
Alexander Kazan,
Managing
Director for
Global Strategy
at Eurasia Group
and one of the
authors of the
report said,
“There is a
clear
humanitarian and
ethical case for
supporting the
ACT Accelerator
and the Covax
facility, along
with the obvious
economic gains
it would bring
to developing
countries; doing
nothing risks
reversing years
if not decades
of economic
progress. But
our analysis
shows that the
program is
likely to yield
economic and
other returns
for major donor
countries as
well. The ACT
Accelerator is a
unique
opportunity to
save lives,
repair the
global economy,
and build
diplomatic
capital that
will last a
generation.”
Hassan Damluji,
Deputy Director
at the Bill &
Melinda Gates
Foundation,
commenting on
the report’s
findings said,
“The moral case
for an equitable
global solution
to the COVID-19
crisis has
always been
clear, but with
high-income
countries
reeling from a
huge shock,
their
governments are
increasingly
focusing on
investments that
can help their
own economies to
rebound. This
report adds to
the body of
evidence that
shows that the
ACT Accelerator
is precisely one
of those
investments. It
is both the
right thing to
do, and an
investment that
will pay
dividends by
bringing the
global economy
back from the
brink,
benefiting all
nations.”
Vaccine Efficacy
May Be Short
Term
A new study by
the New
England Journal
of Medicine (NEJM)
and reviewed by
William
Hazeltine in
Forbes
suggests
that the
long-term
efficacy of
Moderna’s
mRNA-1273
vaccine,
specifically the
neutralizing
antibody count,
may be less than
we were hoping
for.
This
potential adds
to the urgency
to make CATER
masks widely
available and
utilized.
Neutralizing
antibodies bind
to invading
pathogens, like
all antibodies
do, but they
bind in a manner
that stops
infection. That
is why
pharmaceutical
companies stress
neutralizing
antibody counts
as an essential
measure for
their vaccines’
success.
The NEJM study
followed a group
of 34 patients
who had taken
both doses of
mRNA-1273 and
analyzed their
antibody counts
from the
administration
of the first
dose for 119
days.
Neutralizing
antibodies were
monitored in
subgroups of
18-55 years of
age, 56-70, and
71+, as shown
below.
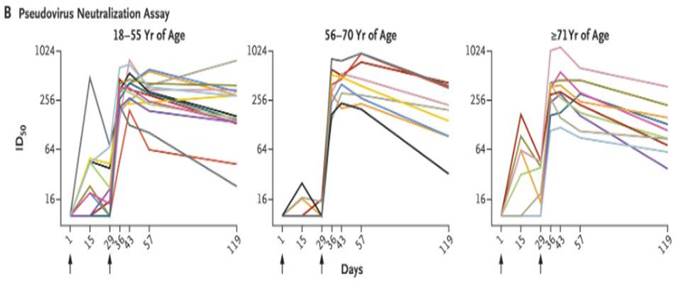
A significant
determinant of
vaccines’
effectiveness in
controlling a
pandemic is
antibody
duration—how
long the
antibodies last
in a person’s
system. For
those 18-55
years old, the
majority only
show a slight
decrease in
neutralizing
antibodies in
the three months
following their
second vaccine
dose. Two of the
34 patients in
this age group
saw a
significant drop
in neutralizing
antibodies. Due
to the limited
number of
participants in
this study, we
cannot draw
conclusions from
these outliers
until further
data becomes
available.
However,
sustained
antibody counts
are not the case
in the 56-70 and
71+ age groups.
In these
subsets, the
neutralizing
antibody counts
fall anywhere
between 50 and
75 percent. This
suggests that in
these age
groups, the
duration of
neutralizing
antibodies from
the Moderna
vaccine will be
relatively
short,
potentially less
than a year.
That is
particularly
troubling as
these are the
age groups most
affected by
severe Covid-19.
It may well be
that the levels
of antibodies
after three
months, if
maintained, are
sufficient to
protect these
age groups, but
it is unlikely
they will
continue to
protect if
levels fall
still further.
Moderna is
simultaneously
producing
vaccines for
avian influenzas
H10N8 and H7N9.
These two
vaccine
candidates show
similar drops in
neutralizing
antibody counts
to mRNA-1273
after three
months.
According to
data from Science
Direct,
antibodies
persisted up to
six months after
injection, but
dropped as much
as 90% in that
time. Sustained
protection from
the virus
requires
sustained
neutralizing
antibodies, yet
the patterns
indicate that
Covid-19
vaccines may be
more than a
one-time
occurrence.
In addition to
Moderna’s bird
flu vaccines
presenting
similar antibody
trends to that
of the Covid-19
vaccine, early
trials required
them to
discontinue
their 400
microgram dose
due to patient
side effects
like injection
site irritation
and headaches.
The mRNA-1273
vaccine will be
two doses of
.5ml each,
according to
the CDC.
While Moderna
trials did not
note significant
side effects
from vaccine
administration,
some effects may
arise in the
general
population.
This is all not
to say Moderna’s
vaccine is not
effective. Even
at these low
numbers,
antibodies may
still be fully
or partially
protective. That
remains to be
seen.
Additionally,
the NEJM study
only analyzes 34
patients, most
of whom are in
the
18-55-year-old
age group.
Conclusions
drawn from such
small data sets
must be taken
with a pinch of
salt, but we
still need to
take the results
seriously—this
data may be the
first of many
indicators that
vaccines don’t
last as long as
we would hope.
It is also vital
to review
similar data in
the Pfizer and
Biotechvaccines
as it becomes
available. The
United States
government and
the governments
of countries
worldwide seem
to be banking on
the
effectiveness of
these vaccines.
Hazeltine urges
pharmaceutical
companies to be
forthcoming on
their continued
monitoring of
these early
patients and
those who have
received the
vaccine more
recently. As
more data like
this is
released, the
clearer the
picture of these
next several
months of the
pandemic
becomes.
New Virus
Variants in Many
Countries
Japan, Spain,
and France have
found small
numbers of
infections
involving a new,
potentially more
transmissible
variant of the
coronavirus,
most linked to
travel from the
U.K., where it
was first
detected.
The rapid spread
of the variant
led to the
lockdown of
London and
southern England this
week, prompted a
temporary French
blockade of the
English Channel
and resulted in
countries around
the world
barring
travelers from
the U.K. Because
few countries
have the
level of genomic
surveillance that
Britain does,
there is concern
that the variant
may have been
traveling across
the world
undetected for
weeks.
A recent study
by British
scientists found
no evidence that
the variant is
more deadly than
others but
estimated that
it is 56 percent
more contagious.
So far, the
British variant
has been
diagnosed in
seven people in
Japan, the
country’s health
ministry said.
All had either
recently
traveled to the
U.K. or been in
contact with
someone who had.
The discovery in
Japan prompted
the country to
close its
borders to all
new entry by
nonresident
foreigners. The
ban went into
effect at
midnight on
Monday and will
last through the
end of January,
the public
broadcaster NHK
reported.
In Spain, the
variant was
found in the
capital region,
local
authorities said
on Saturday.
Antonio Zapatero,
a regional
health official,
said that four
cases had been
confirmed in
Madrid, while
another three
were being
treated as
suspicious. At
least two of the
cases involve
people who had
recently been to
Britain and then
tested positive
in Madrid, as
well as some of
their relatives.
The first case
of the new
fast-spreading
variant of the
coronavirus was
identified in
France on
Friday,
according to the
French health
ministry.
Officials said
that the patient
was a French
citizen living
in Britain who
had traveled
from London to
Tours, a city in
central France,
on Dec. 19, a
day before the
British
government
imposed a
lockdown
following the
emergence of the
variant.
It is normal for
viruses to
mutate, and most
of the mutations
of the
coronavirus have
proved minor.
The British
variant has a
constellation of
23 mutations,
several of which
might alter its
transmissibility.
Vaccine experts
are confident
that the
available
vaccines will be
able to block
the new variant,
although that
has to be
confirmed by
laboratory
experiments that
are now
underway.
The European
Union’s member
nations are
scheduled to
begin
vaccinating
against the
virus on Sunday
with the Pfizer-BioNTech
vaccine. Hungary began
administering
the vaccine a
day early, on
Saturday.
A few other
concerning
variants have
also been
identified,
including one in
South Africa and
another in
Nigeria.
The U.K. said on
Thursday that it
would ban travel
from South
Africa after the
British health
secretary, Matt
Hancock, said two
people were
confirmed to
have been
infected with
the variant that
emerged there.
Germany and
Singapore have
identified
infections with
the new variant.
And Denmark,
which has wider
genomic
surveillance
than many other
countries,
detected 33
cases of the
variant from
Nov. 14 to Dec.
14, according to
the Danish
health
authorities.
The U.S. has not
yet reported any
cases of the
U.K. variant.
But the
country will
require all
airline
passengers
arriving from
Britain to test
negative for the
coronavirus
within 72 hours
of their
departure, the
Centers for
Disease Control
and Prevention
said Thursday.
The
rule will took
effect Monday,
December 28.
Holistic Plan to
Battle COVID for
1.7 Billion
Students
There are now
nearly 1.5
billion children
around the globe
— or 87 percent
of Earth’s
student
population —
whose schools
have closed
because of the
novel coronavirus pandemic,
and more than 60
million teachers
are home as
well, according
to a United
Nations agency.
Schools in
nearly 165
countries have
shuttered,
There are
140,000 schools
in the U.S.
|
Level and control of institution |
2012–13 |
2013–14 |
2014–15 |
2015–16 |
2016–17 |
|
Public schools |
98,454 |
98,271 |
98,176 |
98,277 |
98,158 |
|
Elementary |
66,708 |
67,034 |
67,073 |
66,758 |
66,837 |
|
Secondary |
24,294 |
24,067 |
24,181 |
24,040 |
23,814 |
|
Combined |
6,329 |
6,189 |
6,347 |
6,788 |
6,783 |
|
Other |
1,123 |
981 |
575 |
691 |
724 |
|
Private schools |
– |
33,619 |
– |
34,576 |
– |
|
Postsecondary Title IV institutions |
7,253 |
7,236 |
7,151 |
7,021 |
6,606 |
|
Degree-granting institutions |
4,726 |
4,724 |
4,627 |
4,583 |
4,360 |
|
2-year colleges |
1,700 |
1,685 |
1,616 |
1,579 |
1,528 |
|
4-year colleges |
3,026 |
3,039 |
3,011 |
3,004 |
2,832 |
Each school can
be viewed as a
potential
bubble.
The big
universities
with 10,000
students would
be large
bubbles. The
average school
in the U.S. with
700 students
would be a much
smaller bubble.
The universities
in developed
countries have
all the
technical
capability to
conduct fitness
tests and
monitor the use
of them in their
buildings.
Many of the 1.7
billion students
are in
environments
where fitness
testing and
funds for masks
will have to
come from
wealthy
countries.
In the Alert
yesterday we
cited studies
which showed
that if
the 67 poorest
countries do not
contain the
virus in the
next year the
cost to the 10
wealthiest
countries will
be $350 billion.
Mask programs
for students can
therefore be
justified just
on the selfish
interest of the
wealthy
countries.
![]()