Coronavirus
Technology Solutions
November 20, 2020
Herd Immunity with a Combination of Vaccines and
CATE Masks
Three Million Americans are Now Infectious
Purifan Ceiling Filter is Being Sold to Homes, Schools, and Bars
_________________________________________________________________________
Herd Immunity with a Combination of Vaccines and
CATE Masks
Future cases of COVID can be determined
by the reproduction number (RO
pronounced “R
naught”)
In the case of measles in an unvaccinated
population it is a high as 18. Each infected
person infects 18 others. Herd immunity occurs
when the RO is below 1 as is the case when most
people are vaccinated.
Presently the RO for COVID in some
countries is as high as 3. The calculation is
that when herd immunity reaches 70% the disease
will start disappearing.
There are a number of variables relative to
immunity through vaccines including the
efficiency and length of protection. Given the
recent announcements relative to vaccines we can
guesstimate that 20% of the world population
could be vaccinated by July 1. Over the
following year the percentage could increase to
65%.
|
Number of People Vaccinated Worldwide |
|
|
Date |
Cumulative % |
|
July 1, 2021 |
20 |
|
October 1, 2021 |
40 |
|
January 1, 2022 |
50 |
|
April 1, 2022 |
60 |
|
July 1, 2022 |
65 |
Mask use can compensate for the lack of vaccine
with maximum deployment in the next six months
and then steady reduction over the next 20
months. Many people will refuse to take the
vaccine. In poorer countries it is unlikely that
the 65% vaccination level can be obtained in the
next two years.
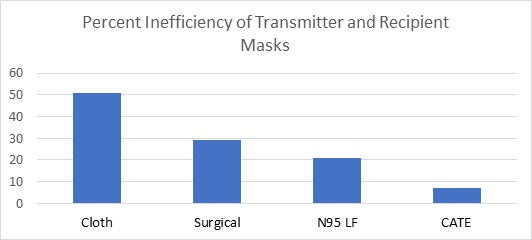
It is important to understand the big
differences between masks.
CATE is an acronym
for Comfortable, Attractive, Tight Fitting,
Efficient. These masks have been available for
many years to combat air pollution, wildfires
and pollen. They are the ideal selection for the
general public in the fight against COVID. This
is not true of other mask types. Here are the
numbers.
In a room where
people are social distancing at six feet and
MERV 8 filters are used in an HVAC system with
three air changes per hour unmasked individuals
will be generating a cloud of virus particles
similar to perfume or cigarette smoke. If masks
are worn by transmitters as well as recipients,
the net protection is a combination of the
performance of both masks.

The net effectiveness
is a function of the potential capability of the
mask minus failure to achieve a tight fit and
periods where the mask is discarded due to
discomfort or social drivers. When all is
considered the CATE mask combination is 93%
effective compared to only 49% for the cloth
mask.
Mask type: CATE masks
are generally reusable and have various features
to make them attractive, tight fitting and
comfortable as well as efficient. Surgical masks
are efficient but not tight fitting. N95 masks
can be fitted for a tight seal but when worn by
general public they are often not used properly.
Cloth masks can excel in comfort and
attractiveness but are loose fitting and
inefficient.
Direct Leakage: This
is the amount of air which is exhaled around the
mask directly.
Re-entrainment:
Droplets initially captured on masks evaporate
and split causing virus to escape.
Penetration: This
relates to the efficiency of the filter media.
Use Discount: Masks
should be worn as appropriate. Cloth and CATE
masks are more comfortable than the others and
are more likely to be used in borderline
situations.
Recipient Load: This
is the virus escaping the transmitter mask.
In Leakage: This is
the amount inhaled around the mask seals.
There is no question
that tight fitting efficient masks are the most
effective weapon against COVID. These masks
prevented any U.S. medical staff fighting
Ebola to become infected. The COVID incidence
among medical personnel in high COVID
environments is very low. In cases where these
personnel had no choice but loose fitting
surgical masks the infection rate was high. If a
comfortable, attractive version is available to
the general public the battle can be easily won.
So combining CATE masks and vaccines is a
winning combination.
CATE
masks have a 7% inefficiency factor. So when 20%
are vaccinated you need 57% wearing masks to
reach the 70% herd immunity.
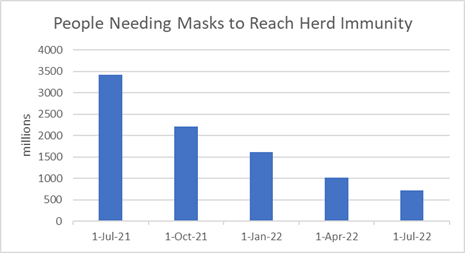
If 6 billion of the 8 billion people in
the world need to be masked or vaccinated then
3.4 billion people will need masks through July
of next year. This number decreases over the
next 12 months to just 720 million people.
(These estimated do not take into account
the people who are immune because they were
infected.
Nor those who take the vaccine but are
not immune. These may not be entirely
offsetting.)
|
Date |
Cumulative % Vaccinated |
Mask Inefficiency |
% needing masks |
People Needing Masks millions |
|
July 1, 2021 |
20 |
7 |
57 |
3420
|
|
October 1, 2021 |
40 |
7 |
37 |
2220 |
|
January 1, 2022 |
50 |
7 |
27 |
1620 |
|
April 1, 2022 |
60 |
7 |
17 |
1020 |
|
July 1, 2022 |
65 |
7 |
12 |
720 |
Because CATE masks are reusable it is not an
insurmountable challenge to supply masks for
billions of people. Longer term the market could
fall to 720 million people wearing three masks
per year at $30 per mask or $64.8 billion.
This does not include masks needed for
air pollution, pollen, and wildfire protection.
The technical analyses of masks and filters are
found in Coronavirus Technology Solutions
Click here for more information
Custom market research is also available. Bob
McIlvaine can answer your questions at 847 226
2391 or
rmcilvaine@mcilvainecompany.com
Three Million Americans are Now Infectious
More than three million people in the United States have active coronavirus infections and are potentially contagious, according to a new estimate from infectious-disease experts tracking the pandemic. That number is significantly larger than the official case count, which is based solely on those who have tested positive for the virus.
According to an article today in the Washington Post, the vast — and rapidly growing — pool of coronavirus-infected people poses a daunting challenge to the governors and mayors in hard-hit communities who are trying to arrest the surge in cases. Traditional efforts such as testing, isolation of the sick and contact tracing can be overwhelmed when a virus spreads at an exponential rate, especially when large numbers of asymptomatic people may be walking around without even knowing they are infectious.
To put the 3 million-plus figure in perspective: It is close to 1 percent of the population. It is about equal to the number of public school teachers in the entire country, or the number of truck drivers. If the University of Michigan’s football stadium were packed with a random selection of Americans, about a thousand of them would be contagious right now.
Columbia University epidemiologist Jeffrey Shaman said his team’s model estimated that 3.6 million people are infected and shedding enough virus to infect others. That’s a 34 percent week-to-week increase that followed a 36 percent increase in the previous seven-day average, he said.
The estimate does not include
an approximately equal number of latent
infections among people who caught the virus in
recent days and can’t pass it on yet because it
is still incubating.
It’s bad; it’s really, really bad,” Shaman said. “We’re running into Thanksgiving now and that’s only going to make it worse. We’re going to go through a lot of people being infected between now and the end of the year, unfortunately.”
Separately, modelers at the University of Washington’s Institute for Health Metrics and Evaluation estimated Tuesday that approximately 3.2 million people have been infected just since Election Day, Nov. 3, a figure significantly larger than the approximately 1.95 million official cases tracked over the same period by The Washington Post through reports from state health departments.
When do you want to hit the brakes? That’s the
question,” said Ali Mokdad, an epidemiologist at
IHME who is among many scientists and doctors
urging action by the government and general
public to reverse the trend lines. “When you
have a fire, you send the firetruck. You don’t
wait and say, ‘Okay, let me wait a little bit,
maybe that fire isn’t going to spread that
much.’ . . . We already moved into exponential
growth. Just hit the brakes as soon as you can.”
This fall wave of infections and
hospitalizations is different in several ways
from the one last spring. The outbreaks are
widespread now, with 49 states showing rising
coronavirus hospitalizations, in contrast to the
spring’s concentration of cases in the Northeast
and a few large cities. Doctors are better at
treating severe cases of covid-19, the disease
caused by the virus, and so it is less likely to
be fatal.
But the biggest difference is that this fall
wave is still swelling and is probably many
weeks from cresting. This pandemic is following
the seasonal pattern of the 1918 influenza
pandemic, the worst such plague in U.S. history,
in which the autumn wave was worse than the
first one in the spring of that year. Even after
more than 11 million confirmed infections since
early in the year, more than 8 in 10 people in
the United States remain susceptible to the
coronavirus, experts estimate.
The non-tested cohort includes people who have
no symptoms but will in coming days. It also
includes people who will never develop symptoms.
And it includes people who have symptoms but
don’t want to deal with the consequences of a
positive test, such as being forced to miss work
or become isolated from their social network.
What happens next depends on public awareness of
the reality of the emergency and the willingness
of state and local officials to respond in a
manner commensurate with the crisis while also
acceptable to people suffering from pandemic
fatigue.
Despite lower mortality rates, the dramatic rise
in infections that began in September has seen a
delayed echo in the rise of the death toll. More
than a thousand people are dying daily on
average, and the country is nearing 250,000
deaths since the start of the pandemic.
Although the surge of infections this fall has
in some measure been due to colder weather and
people congregating indoors, it has also been
because of human behavior — specifically, the
willingness of millions of people in the United
States to ignore public health guidelines on
facial coverings and social distancing. What is
happening across the country is not inevitable,
experts say.
The current strategy in many states — patchwork
restrictions, combined with widespread public
disregard of public health guidelines — portends
a brutal winter for the country in which
hospitals could be strained to their limits or
beyond, something that is already happening in
the Dakotas and other communities of the Upper
Midwest and Great Plains, as well as El Paso.
“We’re getting the herd immunity strategy
whether we want it or not,” said Andrew Noymer,
an epidemiologist at the University of
California at Irvine. “We have a totally out-
of-control epidemic and we are taking baby
steps.”
The only period comparable to the current one in
terms of the size of the infected cohort was in
late March and early April. Tests were hard to
come by early in the pandemic. Robert Redfield,
director of the Centers for Disease Control and
Prevention, estimated that the number of
infected people was 10 times the official count.
Now the multiplier is surely lower — the model
developed by Columbia University researchers
uses 5.5. By that measure, as many as 10 million
people in the United States have been infected
in the past two weeks.
Researchers at IHME estimate the number of daily
new infections by working backward from the
known numbers of deaths. The institute relies on
an estimated infection fatality rate of 0.6
percent across all populations, Mokdad said.
These are models, and they rely on a series of
assumptions about a virus for which much remains
unknown — including how long, exactly, a person
who is infected will remain contagious.
But the big picture is clear.
“We’re going in the wrong direction,” Shaman
said.
Purifan Ceiling Filter is Being Sold to Homes,
Schools, and Bars
The Purifan five-layer filter captures
particulates and odors using EPA-recommended
filtering media technology. It uses recycled
paper, HEPA-level particulate filters, and there
is activated charcoal in three of the five
layers. There are no electrically-charged
particles put into the air, and no free-floating
ions or Ozone added to the room.
Purifan’s
filtration system contains a polyester
pre-filter to capture large particles like pet
hair, dust, and carpet fibers. The second layer
is an activated carbon filter, which absorbs
odors and gases, then there’s a nanoparticle
filter which al so has activated carbon to
further capture odor-causing particles. The
nanoparticle media consists of activated
charcoal that has been crushed only a few
nanometers in diameter, increasing its
odor-absorbing surface by 10,000 times. The
fourth layer is a HEPA filter, which traps
particles as small as .3 microns, and the final
layer is another activated carbon filter, which
gets rid of any remaining pollutants or odors.
Purifans
in a 20 x 40 foot classroom
·
Total installed cost for two Purifans and motors
= less than $1,200 (about $60 per student one
time)
·
Two filter changes per year for each unit = $180
total (about $9 – $10 per student annually)
·
One school using Purifans reported the average
student took 11 fewer sick days per year. For
parents, their employers, teachers, and
administrators, that’s worth far more than $10
per year.
·
Bars
and Clubs
-
Part of the total cost of owning
a smoke and odor solution is the
operating expense. One
electrostatic smoke eater can
add $300 or more to a club’s
monthly electricity bill, and
many clubs have multiple units.
The energy-efficient Purifan is
totally silent and uses only
half an amp of electricity, the
same as a 60-watt bulb, even
when running on high. Compare
this to electrostatic models
which are loud and can draw 8 to
10 amps when operating on high.
-
Low Maintenance Costs
Just on monthly maintenance alone, Purifans can save a lot of money for the bar or club. Most electrostatic smoke removal solutions require monthly cleaning, and typically require expensive repairs after only a couple of years. All that’s needed to keep a Purifan running like new is regular filter changes. There’s no cleaning needed because the filters are disposable. There are no tools required, and you can change the filter yourself in minutes. Depending on the number of units in a room and the density of smokers, Purifan filters last three or four months, and longer when smoking levels are lower during slow business periods.
Purifan announced a new optional upgrade package
that adds a Purifan Certified UVC Germicidal
Light Kit to kill viruses quickly when
aerosolized droplets are captured in the five-
stage filter system. Purifan’s Ceiling Mounted
Air Filtration Systems have been removing tiny
particles and smoke from the room air since
1998. Over 50,000 have been installed, mostly
through customer referrals.
Upgraded with a UVC 253.7 nanometer Germicidal
light, the Purifan kills any live viruses,
bacteria or germs in a few minutes of exposure.
Many scientists and research groups have
published studies that report COVID19 can also
be spread in public places, by the microscopic
moisture droplets that can float in the air in
the room for an extended time. This happens in
offices, nursing homes, businesses, classrooms,
stores, day cares, bars and restaurants. These
microscopic droplets are created by normal
exhaling, talking, singing, yelling, coughing or
sneezing, and some of these moisture droplets
attach to floating dust particles in the air.
Then these droplets can be inhaled or deposit on
the surface of the eyes to infect the healthy
people in the room up to 20-30 feet away.
Tracking studies on COVID spread have shown
these particles emitted by a contagious person,
drift freely on air currents in the room.
Tracking investigations showed that people in
the room can be infected more than 20 feet away
from the sick person.

Purifans are powerful air filtration systems
that mount to the ceiling, exactly like a normal
ceiling fan. A single Purifan typically filters
all the air in a 20 x 20 x 8 foot area once
every 90 seconds. Purifans produce a powerful
2,200 CFM airflow pattern pulling the moisture
droplets and other airborne particles or smoke
up and into their five stage filter system,
capturing the moisture droplets in the filters.
Once the moisture droplets are captured in the
Purifan filters they dehydrate, and the risk of
aerosolized spread is substantially reduced or
eliminated. Purifans use disposable 5 layer
filters including .3 micron paper filter media
and activated charcoal filter media to capture
particulates, odors and Volatile Organic
Chemicals. Filters are replaced 3 or 4 times per
year in most office or business applications.
Filters are replaced two times per year in a
typical classroom. Purifans produce no ozone or
ionic particles that are considered unhealthy to
people in the room.
Purifan option UVC Light Kit Upgrade shines a
proven virus-killing, UVC 253.7 nanometer,
germicidal light onto the surface of the filters
in the Purifan, killing any live viruses,
bacteria or germs in a few minutes of exposure.
The very specific 253.7 wavelength of UVC light,
interacts with the DNA of any virus or bacteria
and damages its ability to replicate and
survive. Purifans use these UVC Germicidal
lights to kill viruses and bacteria on the
surface of the filters. There are many proven
uses of UVC light to disinfect areas like
hospital rooms, surgery areas and doctors’
offices.
Purifans are silent, high-capacity, ceiling
mounted air filtration systems that filter a 20
by 20 foot area, 40 times per hour to reduce the
number of airborne fine particulates by 90% or
more.
In addition to thousands of Purifan
installations in bars and Veterans Clubs, homes,
offices, and businesses, Purifans have been
installed in classrooms in over 50 schools
starting in 2005. In every case, the teachers
and students saw a significant reduction in
missed school days due to the spread of seasonal
colds and flu, which have similar spread
patterns like COVID19.

After Purifans were installed in classrooms and
hallways, reported attendance records of some of
these schools reported the following:
·
the annual missed school days for children was
reduced by as much as 61%,
·
teachers had 50% fewer sick days,
·
a 70% reduction in children needing to use their
inhaler based on logs kept at the school nurse’s
station.
Scholastic test results also improved
dramatically for the children in these Purifan-equipped
schools because the children missed fewer sick
days and they were able to keep up with
classwork. Parents and teachers also reported
many children were able to stop taking mind-
numbing allergy medications they needed daily
before the Purifans were installed.
Schools reported up to a 61% reduction in
student sick days, a 50% reduction in teacher
sick days and a 70% drop in inhaler use by
students.
Purifan management believes the entire cost of
installing Purifans and changing the filters and
UVC lights in elementary school classrooms will
be recovered by the substantial financial
payback to Medicaid Health Costs for Children.
Since the annual savings far exceed the costs,
the company believes that Medicaid Insurance
Program or other designated Federal Funding
should pay for the installation, and the
expendables cost for filters and the new UVC
germicidal bulbs. The projected payback is
typically calculated at over 20 to 25 times the
cost. That payback does not go to the school’s
budget, it goes to Medicaid, private health
insurers, the families, and their employers. The
savings comes from reduced health costs for the
Medicaid insured children in the classrooms.
When Purifans filter allergens out of the school
air, allergy and Asthma related health costs to
Medicaid are substantially reduced. Now with the
potential
Purifans are also suited for Retail Stores,
Pharmacies, Waiting Areas. They are quiet,
overhead and out of the way.

Purifans will help Medicaid-insured children to
have reduced needs for doctors visit, testing,
prescription drugs, inhalers and other more
serious health issues like Asthma or a
COVID-like infection and hospitalization. This
can save Medicaid more than 25 times the cost of
funding the Purifans in schools on an annual
basis.
Purifans are ideal for many small businesses,
stores, pharmacies, barber shops, hair and nail
salon, retail stores, dry cleaners, waiting
rooms, gyms, day cares and office areas, where
the goal is to protect the employees, and make
the customers feel like everything is being done
to reduce the risk of aerosolized spread of
COVID 19.
![]()